

Introduction
Essential thrombocythemia (ET) and polycythemia vera (PV) patients suffer from various symptoms that worsen quality of life (QOL), yet serial data on symptom changes resulting from therapy are sparse in the literature. Patient questionnaires from 2 large multicenter trials (MPN-RC 111, 112) were used to assess change in symptom burden and QOL over 12 months and impact of baseline symptom burden on subsequent change in ET / PV patients on hydroxyurea (HU) or pegylated interferon alfa-2a (PEG).
Methods
Trials
MPN-RC 111 was a single-arm, open-label, phase II trial evaluating response to PEG in high-risk ET / PV patients with HU resistance/intolerance or splanchnic vein thrombosis (SVT; NCT01259817). MPN-RC 112 was a randomized, open-label, phase III trial comparing response to PEG versus HU in cytoreductive therapy naïve high-risk ET / PV patients diagnosed < 5 years ago (NCT01258856).
Measures
Patients reported disease-related symptoms via the validated Myeloproliferative Neoplasms Symptom Assessment Form (MPN-SAF), QOL via the European Organisation for the Research and Treatment of Cancer Core QOL Questionnaire (EORTC QLQ-C30), and (if applicable) PEG-related symptoms (flu-like symptoms, injection site irritation, blurry vision, vision change, flushing) at baseline, 3, 6, 9, and 12 months.
Analysis
Mixed models assessed mean changes from baseline in the MPN-SAF Total Symptom Score (TSS), MPN-SAF items, QOL, and PEG-related symptoms in MPN-RC 111, 112 PEG, and 112 HU patients. Mixed models also assessed the impact of baseline symptom burden (high [TSS ≥ 20] versus low) on subsequent change in PEG (MPN-RC 111 and 112) and HU patients.
Results
Patients
Of the 135 enrolled MPN-RC 111 patients, 20 with SVT and 1 with no questionnaires were excluded. Of the remaining 114, 64 (56%) / 50 (44%) had ET / PV. Patients were 51% / 48% female. Median age was 65 / 64 years, and median time since diagnosis was 38 / 55 months. 31% / 22% had prior thrombosis, and 19% / 56% had splenomegaly.
Of the 168 enrolled MPN-RC 112 patients (82 PEG, 86 HU), 2 with no questionnaires were excluded. Of the remaining 166, 79 (48%) / 87 (52%) had ET / PV. Patients were 50% / 33% female. Median age was 60 / 62 years, and median time since diagnosis was 3 / 3 months. 25% / 29% had prior thrombosis, and 11% / 37% had splenomegaly.
Symptoms
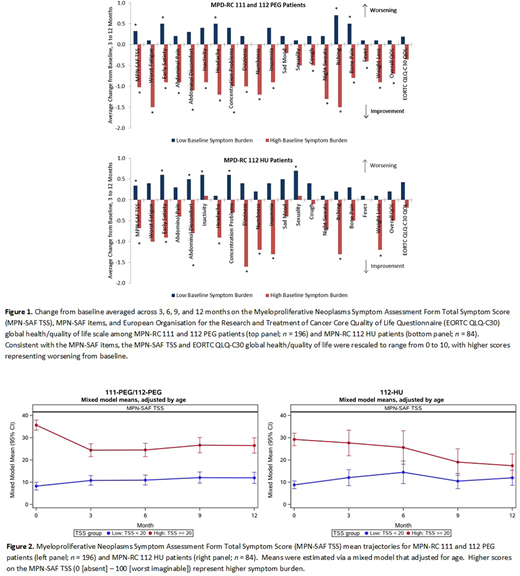
Questionnaire completion rates ranged from 90 - 99%, 87 - 100%, and 75 - 96% for on-treatment MPN-RC 111, 112 PEG, and 112 HU patients. At baseline, TSS (0 [absent] - 100 [worst imaginable]) and QOL (0 [very poor] - 100 [excellent]) means (SDs) were 19.5 (18.4) and 71.6 (20.1) for MPN-RC 111, 17.0 (13.6) and 67.9 (24.3) for MPN-RC 112 PEG, and 14.6 (11.4) and 73.8 (18.8) for MPN-RC 112 HU patients. On average, MPN-RC 111 patients had significant improvement of TSS, fatigue, abdominal pain, abdominal discomfort, dizziness, numbness, night sweats, and fever; MPN-RC 112 PEG patients had significant worsening of fever; and MPN-RC 112 HU patients had significant worsening of inactivity (no mean changes indicating improvement were observed). PEG patients had significant worsening of PEG-related symptoms.
The greatest improvements occurred in the 46 (40%), 27 (33%), and 23 (28%) MPN-RC 111, 112 PEG, and 112 HU patients with high baseline symptom burden. On average, PEG patients with high baseline symptom burden had significant improvement of TSS, fatigue, early satiety, abdominal pain, abdominal discomfort, inactivity, headache, concentration, dizziness, numbness, insomnia, cough, night sweats, itching, bone pain, fever, weight loss, and QOL, while those with low baseline symptom burden had significant worsening of TSS, early satiety, headache, itching, and bone pain. On average, HU patients with high baseline symptom burden had significant improvement of TSS, early satiety, abdominal discomfort, headache, dizziness, numbness, insomnia, itching, and weight loss, while those with low baseline symptom burden had significant worsening of TSS, early satiety, abdominal discomfort, inactivity, concentration, and sexual desire/function (Figures 1 and 2).
Conclusions
Although no statistical comparisons were made across trials, overall improvements were seen in MPN-RC 111 but not 112. Patients with high baseline symptom burden experienced the greatest improvements in symptom burden and QOL during treatment with PEG or HU, which may explain the improvements seen in the more advanced patients in MPN-RC 111 compared to 112.
Mascarenhas:Celgene, Prelude, Galecto, Promedior, Geron, Constellation, and Incyte: Consultancy; Incyte, Kartos, Roche, Promedior, Merck, Merus, Arog, CTI Biopharma, Janssen, and PharmaEssentia: Other: Research funding (institution). Yacoub:Dynavax: Current equity holder in publicly-traded company; Ardelyx: Current equity holder in publicly-traded company; Cara Therapeutics: Current equity holder in publicly-traded company; Hylapharm: Current equity holder in private company; Incyte: Speakers Bureau; Agios: Honoraria, Speakers Bureau; Novartis: Speakers Bureau; Roche: Other: Support of parent study and funding of editorial support. Hoffman:Protagonist: Consultancy; Forbius: Consultancy; Novartis: Membership on an entity's Board of Directors or advisory committees; Abbvie: Membership on an entity's Board of Directors or advisory committees; Dompe: Research Funding. Silver:PharmaEssentia: Speakers Bureau. Mesa:Bristol Myers Squibb: Research Funding; Incyte: Research Funding; AbbVie: Research Funding; Samus Therapeutics: Research Funding; Genentech: Research Funding; CTI BioPharma: Research Funding; Promedior: Research Funding; Sierra Oncology: Consultancy; LaJolla Pharmaceutical Company: Consultancy; Novartis: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal